buzzfeed Press
57 Shocking Hospital Secrets That Would Make Patients Never Want To Set Foot In One Again
Images
1 / 18
2 / 18

3 / 18
4 / 18

5 / 18

6 / 18
7 / 18
8 / 18

9 / 18
10 / 18
11 / 18
12 / 18

13 / 18

14 / 18
15 / 18
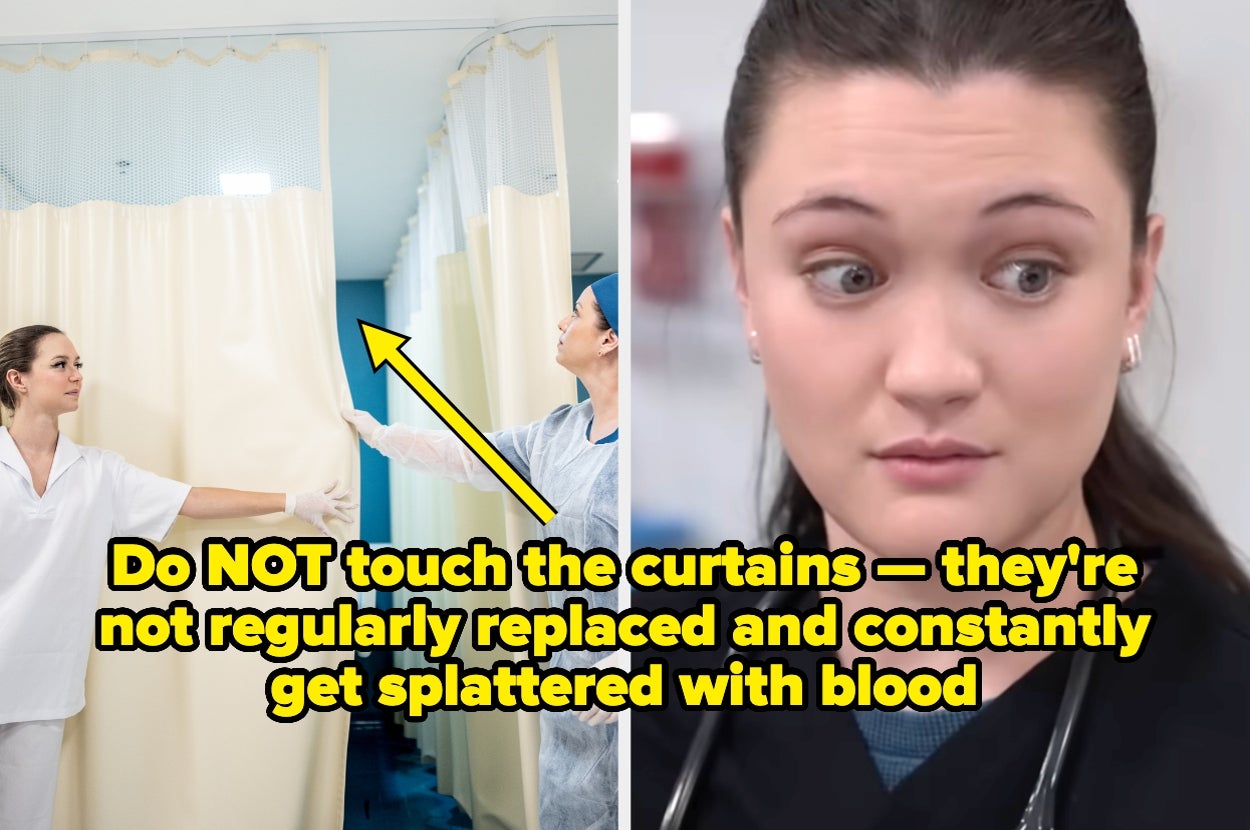
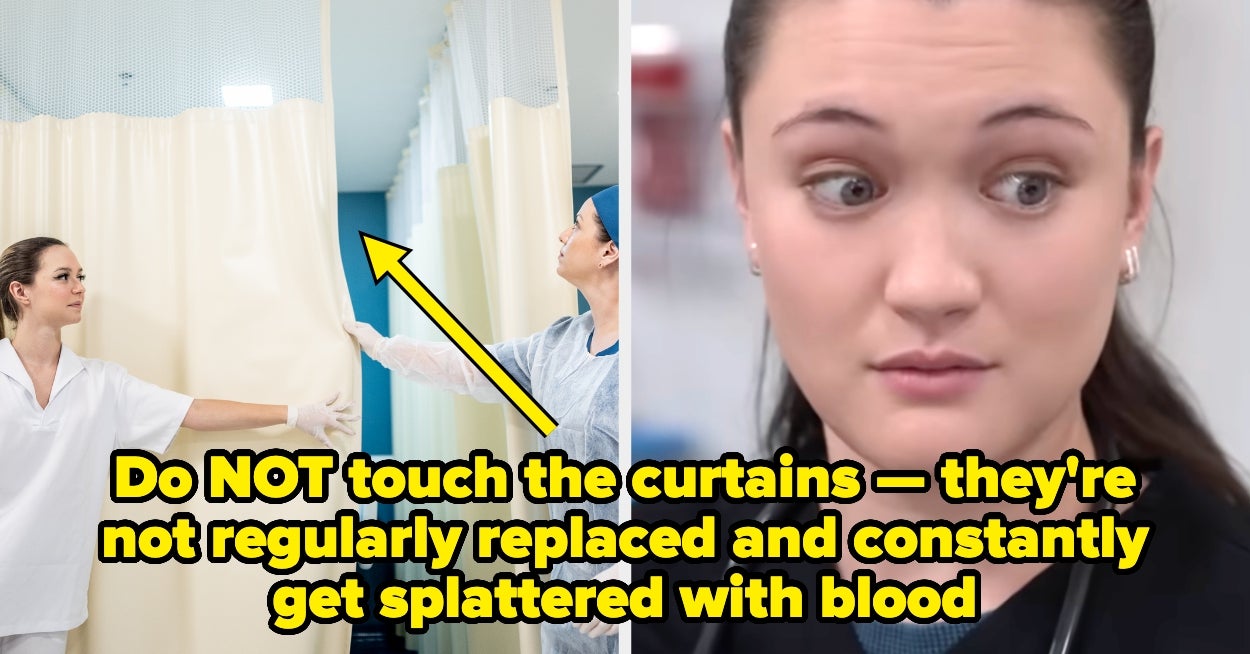
16 / 18
17 / 18
18 / 18
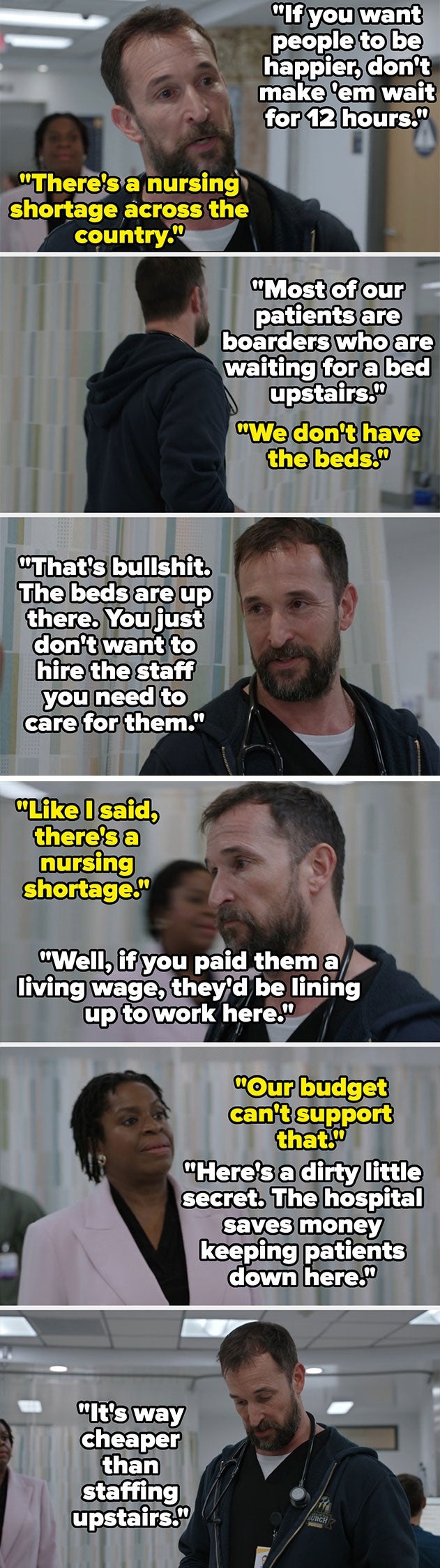
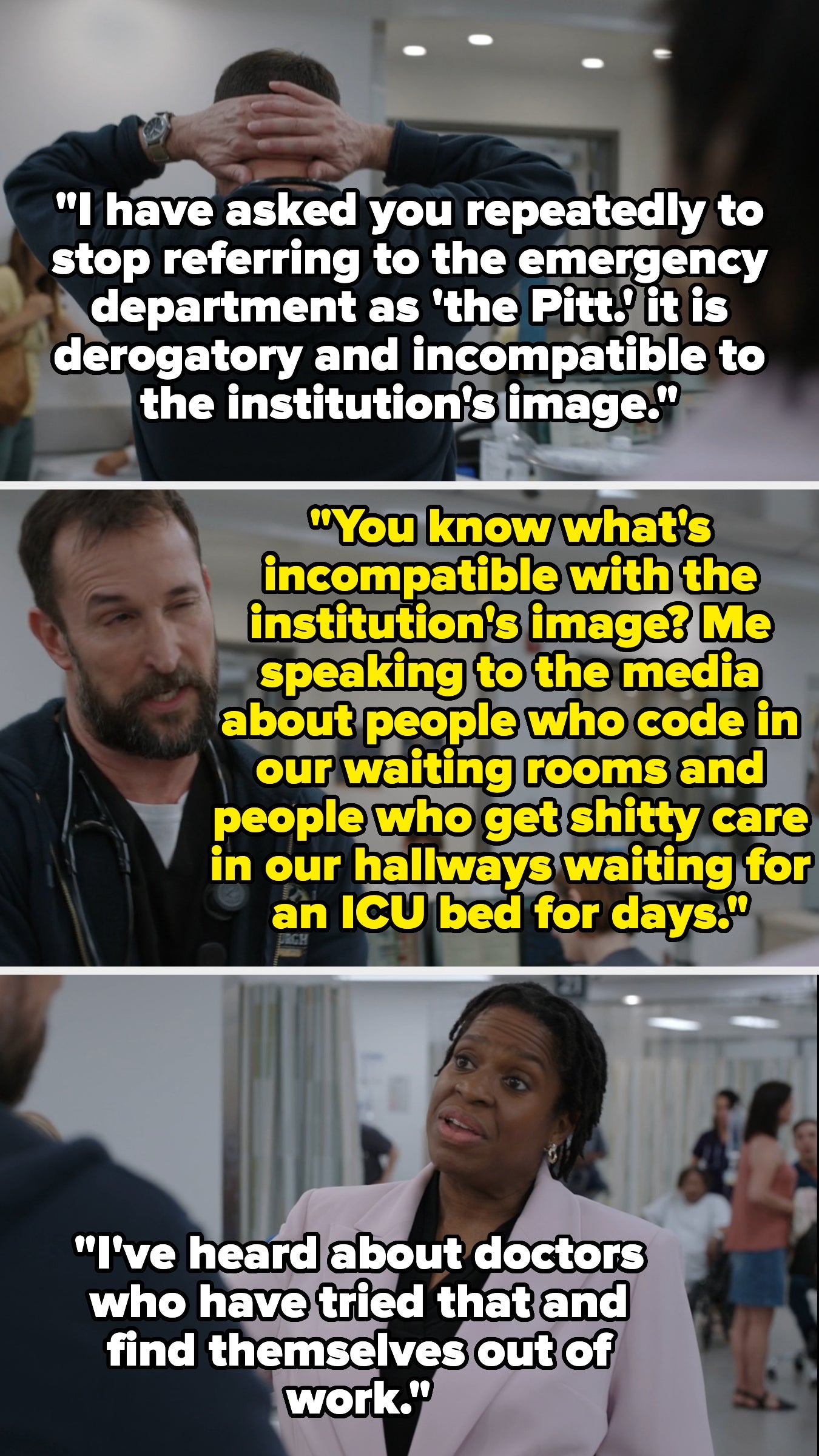
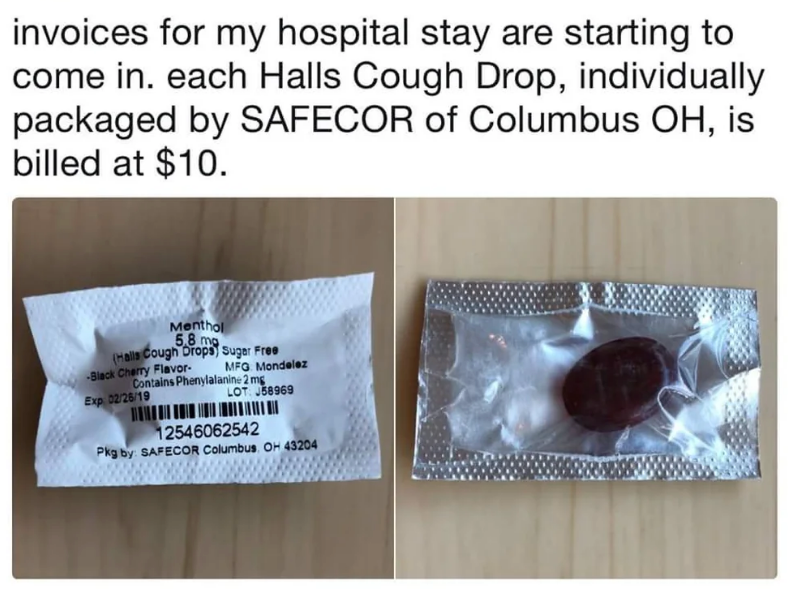
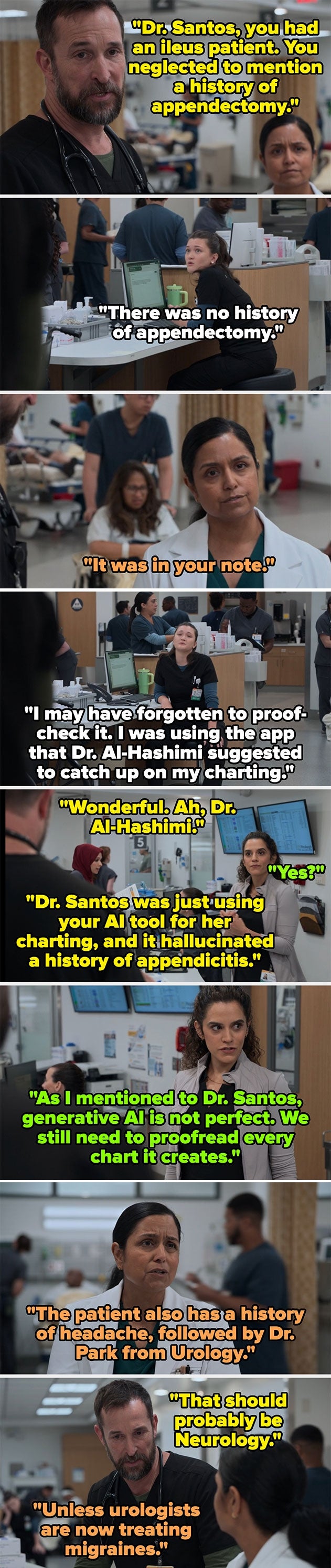
“[Orthopedic surgery is] basically high-stakes construction work where the building can scream.” I'm a Senior Staff Writer based in New York City, where I've been covering classic BuzzFeed-style content since 2020. "It sure is! I actually was part of a group that did a research study and published a paper on EMS handoff. We followed the patient as soon as they were brought into the trauma room, through their outcomes. We observed the handoff between EMS and ED staff and recorded the information that was provided. Then we obtained and reviewed the EMS records to determine what info was provided to EMS at the scene. We found basically what you're describing — that info is often lost in translation or just lost in general due to not having a standardized handoff. For EMS personnel that utilized an implemented handoff tool, and when a time out was called so that the handoff could be completed thoroughly (still less than 30 seconds), reports were more accurate, and patients had better outcomes at hospital release, and after 30 days. " "I remembered this lesson as a young nurse. Got one patient with a broken leg that was told in the report that he was basically a drunken bum found in a train yard. Then, I saw his label said work comp; turns out he was a train conductor who had an accident, and his ED drug screen showed nothing." "Imagine a patient on insulin. The doctor prescribes and sends the prescription to the pharmacy. Pharmacist verifies. The technician will run it up to the floor. The nurse administers. Every step in that process could be completely arbitrarily delayed, sometimes up to hours at a time. Even on a good day. The only drugs that were consistently on time at my old hospital were the pain meds, and I still think that's only because the nurses were worried about *themselves* listening to patient complaints." "The red mist in the room during hip and knee replacements. " "I couldn’t eat the chicken fingers in the cafeteria because they smelled like cautery. " "People think surgeons use futuristic laser scalpels for everything. In reality, half of an orthopedic surgery sounds like a Home Depot workshop. There’s a lot more literal hammering, sawing, and 'I think we need a bigger bolt' than anyone tells you. It’s basically high-stakes construction work where the building can scream." "I regularly have to wipe blood smears off of 'clean' hospital beds because the cleaning staff isn't thorough about the stirrups." "Isn’t it great when you break apart a bed in front of a patient and find body fluids, and you have to very casually and discreetly clean it?" "I briefly worked with a midwife in a vaccination center, and she told me there was a room that had a horrible smell for weeks. Then one day, someone opened a compartment under the bed and found it full of rotting bodily fluids." "Those cardiac leads have seen thousands of patients and don’t get anything more than one pass with a sanitary wipe between a bloody mess or a shit-filled gurney. " "Hospital rooms are usually extremely unhygienic. They pay someone barely above minimum wage to clean hospital rooms for five minutes. They don’t clean most surfaces between sick patients." "I clean at a hospital, and they do not care about how detailed the rooms are cleaned. They are more worried about rooms being flipped fast so they can transfer patients up so they can start billing their insurance. " "The amount of drug-resistant microbes. Heard a story from my Principal Investigator (clinical research team leader) that a research group was trying to publish some shocking results, and then got shut down by the hospital, and the hospital admin threatened legal action." "This is how my uncle died. He was actively dying at home, so we finally got him to the hospital. They beat his gastrointestinal ailments, only for him to catch an upper respiratory staph infection. Always wonder if he had gone to the hospital a bit less frail (before the GI issues completely made him unable to eat), whether he would have survived the infection." "I watched my ER doc rub his eyes like a toddler after touching the mystery rash near my hip replacement. No gloves. And they wonder why I suffocate/gasping for air under a KN95—cuz y'all nasty." "If my stuff touches the hospital floor, I want to burn it. People are always sitting with their shoes under their butts on the chairs. I do not want the floor germs on my ass. I always clean my chair before my shift or throw a sheet on it if it’s fabric. Most of the day shift people know not to sit in the chair at the space I’ve occupied for the day, but the night crew tends to sit in my chair and put their stuff on it. I’m still logged on and have time left on my shift. For the love of Christmas trees, please pick a different chair." "The lab ran cultures on a tissue sample that was dropped on the OR floor (you know, the room that is supposed to be wall-to-wall sterile), and it grew the most panresistant super bugs I've ever seen" "Do they not get cleaned every time a new patient comes in? 😰" "No. They get replaced every couple of months." "My mom pushed on the bandaid covering her IV site and absolutely fountained blood on the curtain. It just got wiped off a bit. She's just old, nothing transmissible to worry about, but still…" "What's missing in the conversation is that the curtains are made and chemically treated to be antimicrobial. So if a little bacteria finds itself landing on the curtain, it dies." "Add blood, piss, and vomit to the mix. " "Everything has been peed on. Everything. Saturated in urine at some point and scrubbed mercilessly in the hopes the stench will one day go away. Every piece of furniture, every spot on the floor, every wall...Everything." "We had a room sealed off in the ER because of maggots. I asked when the room would be okay to use again — the charge nurse said, 'Oh, we are waiting for Joe to come down. He's the exterminator.'" Imagine my surprise when the ED had its own dedicated exterminator 🙃who was on a first-name basis. (Joe didn't get there quickly enough, and the maggots went on parade. Very fun trying to be a maggot herder and keep the patients unaware.)" "You get an exterminator? Our health region just has housekeeping steam-clean the surfaces and the mattress, and change the curtains. After that, it's back to business. I think people would be terrified to know that despite the cleaning efforts and isolation precautions, bed bugs are still present in the hospital. We've found them crawling randomly on the floor, and even falling from the ceiling. 🤮" "We had this poor, sweet older lady who hoarded animals in her trailer. She was infested with fleas. Apparently, if your infestation is bad enough, they'll live on a human." "This one probably is area-dependent. Cockroaches are generally rare where I live, and I have never seen one in the hospital (only worked five-something years, though). I would change cockroaches for whatever infestation bug is common in your area." "The average health care worker has seen more genitals than Bonny Blue and Ron Jeremy combined. Yours aren't special, or particularly different than anyone else's." "100% on the genitals. Trauma pts have to be stripped and flipped. NO one cares about your DICK!!! No one. (Plus I always throw a gown over it.)" "I'd like to add: Your dick shows up under X-rays. Sometimes obscuring bony anatomy." "This includes teaching hospitals with residency programs — at night, it’s all the teenage doctors in their twenties making the calls. (After being in school for 10 years, I still feel like I’m only 18-19 years old, when in reality, I am a grown adult doctor.)" "The room gets cleaned and turned over pretty quickly after the previous patient dies. I've seen a new patient in the room an hour after I declared the previous patient dead." "I once had a fishing hook get lodged between my fingers, and it still had a worm attached. I swear every doctor, nurse, physical therapist, and janitor came in to take a look before they removed it. This was back in the days before phones had cameras, so more than one person took photos with regular old digital cameras. " "Sometimes you don't even have to be interesting. A neurologist once said I had an 'exemplary' optic nerve and brought three other people into the room to look at my 'textbook, beautiful' backs of my eyeballs." "The United States intentionally misrepresents the material conditions of its citizens. One example is *median income*. Median income is the middle of the data set of income, around 83k. But the *modal* income, the most *common* income in the US, is somewhere between 19k-26k, which, if there's any children in the house...is below the Family Poverty Line." "I once had a patient who lived in a cabin in the woods with no running water or electricity. She had a stove for heat. She got sick and didn't leave her recliner for days, and then the shit and piss accumulated and destroyed her flesh so she *couldn't* leave her chair. Months in hospital followed by months in a SNF. She did finally go home, though." "I used to have to take surgery specimens from the OR to the biopsy lab, which was on the other side of the hospital. One guy came out and said, 'This wouldn't fit in the bin so…yeah,' and just handed me an amputated whole leg in bag." "I had a stay in the hospital due to gallbladder surgery. The doctor talked to me for a bit, and he looked so, so sad. Distraught. I was in pain and recovering from surgery, but I asked him how he was. I’m a little bit older than he was, and my mom instincts kicked in… he said he just had a horrible code blue and really wanted to go home. Poor fellow. I wanted so badly to just give him a hug. I squeezed his hand and watched him walk out like the whole world was on his shoulders… " "Working on a surgical ward, I called the doctor up to review a post op patient who was deteriorating. He took ages to arrive. When he arrived, he said to me, 'Sorry, that took a long time. I was elbow deep inside an eight-month pregnant woman's abdomen who was bleeding out in the ED. Who's the patient you wanted me to review?'" "The important thing about googling things in emergency medicine is to not let the patient see your eyes go wide and hear you say 'uhhhhhh' as you pull out your phone." "As a professor, I used to teach my students that being a scientist (doctor) is not about knowing the answers, but knowing how to find the answers. As a biochemist, I don't have every pathway or structure memorized, but I do know how to search the literature to find it." "The AMA literally holds a meeting every year for physicians to discuss their mistakes (usually for improvement and educational purposes). It's that common, and as a patient, you will most likely never be told your care was the consequence of a mistake." "I used to work at an insurance defense firm. The number of cases they would send just as a heads up that they might sue for malpractice (because they should have) was wild!" "Even the best docs in the world make mistakes, and that's simply a reality of how complex healthcare is. The human body is extraordinarily complex, and every medical test has significant limitations. A simple symptom like dizziness has a hundred different things that can cause it, and it's not possible or feasible to rule them all out — at the end of the day, physicians are playing the odds by looking into the most common diagnoses and ruling out life-threatening issues." "People imagine *just* the emotional distress. A competent young doctor runs into the room, does everything possible, and then fails. They are left with the guilt of the consequence. Reality? That doctor studied for 5-6 years to get to that point and spends tons of time inside and outside of the hospital trying to prepare for these situations while also juggling competency in the more mundane parts of clinical care. They know all the big ones, but this is a special scenario they haven't mastered yet. They could have, theoretically, but there's just too much to prepare for. They take initial actions, call for backup, and then, when the attending physician arrives and takes over, they chew them out for having done the wrong thing in front of around 15-20 people (many of whom will gossip about it later). The patient has a bad outcome, and the resident blames themselves. That resident is exhausted, overworked, and now fully believes that all this work they did for years and years has only led to them not only *not* saving a patient's life but actively harming them. " "It’s not even getting something wrong. It’s doing everything right and still death wins. You still feel guilty and 2nd guess yourself. Very, very few cases have little room for error, relatively speaking. In residency, many attendings will still blame you for the bad outcome even if it wasn't your fault. I pulled out a chest tube in my first year of residency, and the pneumothorax (collapsed lung) came back. I did it the textbook way, under supervision. I was still threatened with having to go up in front of M&M (Morbidity and Mortality conferences) and explain my terrible methodology. In reality, it was just their version of hazing. It just sucks how we treat our healthcare professionals (it's not isolated to doctors; nurses might even be worse at eating their young). I had a really bad outcome last year, and I've second-guessed myself so many times. However, I documented well, and that's what got me through it. Every time I thought, 'Oh, I could have done x or y,' I read the chart, and I explained why I couldn't do it or that the patient declined. We need more listening and validating and less blame in medicine." "For our second, I saw the midwife with a net. She was very accurate and discreet. Don't tell my wife I put this on the internet." "My wife pooped with our first kid. They cleaned it up so fast she didn't even notice. I denied ever seeing anything because it would have mortified her. As if having your legs in the air with your vag spread wide open to a room full of people isn't mortifying already…" "I'm a first-year resident, and this has been the most mind-blowing thing about hospital culture to me so far. It feels like so many people hate their jobs and will do or say whatever to get out of doing them. I've met other residents who are guilty of it too, but lots of times the shit rolls downhill to us." "We recently had a full code in the ICU on a patient over 100 years old. I will haunt someone's ass if anyone ever had me as a full code after a certain point. " "CPR has its place, but that place ain't the 90-year-old patient whose functional capacity on a good day is getting from the bed/couch to the toilet." "The hospice company that managed my dad's care at the end called my brother the morning my dad passed and thanked us for letting them know about my dad's DNR. They also don't like doing CPR on older patients. Stop continuing to make their lives miserable and let them go. Thankfully, my entire family got to spend time with him before he died so everyone could say their goodbyes." "I've noticed that people are now generally aware that ribs will get broken, but feeling an older person's sternum crunch and give way under your hands is a very specific feeling. On one hand (no pun intended), it's reassuring to know you're doing quality compressions, but on the other, crunchhhhhh." "I worked on the cardiac arrest registry for my ambulance service when I was on light duties (fuck back injuries), and out-of-hospital cardiac arrest survival is rare. Survival at 30 days and without neurological compromise is even rarer. It’s a bit of a tricky fine line when it comes to public education — we want people to do compressions and locate a defib if it's available when someone drops in public, but we also want people to be realistic about the odds, and the process for getting an advanced care directive/DNR/ whatever it's called where one lives. CPR on Nana or pops isn't likely to save them, and if they survive the brutal resuscitation process, they aren't going to go on to live a happy, healthy life for another 10 years. I agree that it’s straight-up cruel in many situations. Hold their hand, tell them you love them, and let them go peacefully " "I find they're still generally unaware. My spiel whenever someone says they'd want us to do CPR is to ask them where their knowledge of CPR comes from. It's usually TV and movies. Most won't say that, but will agree a little sheepishly when I specifically say it. From there, I tell them it's nothing like that. We don't push on the chest a few times, dramatically say 'Don't you die on me!', you gasp, and then continue on your adventure as if nothing happened. If we do even a somewhat good job, we're breaking most of your ribs almost immediately. Recovery will be long and painful, and you'll never be as good after CPR as you were before, even after you're 'fully recovered.' Plus, the reason your heart stopped will still be there; we haven't magically fixed that, so chances are good it won't work or will happen again." "We all have a death gallows sense of humor in the OR — definitely a coping mechanism." "It's evolved this way in large part thanks to hospitals looking for cheaper alternatives to physicians (they are justifiably paid more) and for-profit schools (some, if not most, entirely online) whose priority is maximizing tuition dollars. Your nurse practitioner, in some cases, may have never worked at the bedside as a nurse, just gone straight to NP as a new grad with a bachelor’s in nursing. And suddenly they're supposed to be qualified to diagnose and treat. I’m an RN in an urban trauma/teaching hospital and am considered by nature of my position to be one of the top bedside nurses in the facility. I've been doing this for almost two decades, and I genuinely feel that I don’t know enough to practice above the level of an RN. You'd be shocked how often NPs ask me for advice. I definitely know what I’m doing, but I don't have the depth of understanding about why I’m doing it than your physician does." "He does the best he can, but he's not in charge, and the maintenance leadership is more interested in playing political union games and covering their own asses than admitting to problems and getting stuff fixed. My brother says it's very much like how one of our older relatives described communism in Soviet Russia; everyone reports to their superior that everything is fine, so they don't look bad, and that's how it goes up the chain. Senior leadership does essentially the same when reporting to the government, and the cycle of neglect continues. " "We're constantly having issues with the AC/heating because, as one technician told me, it's 'three 20-year-old systems patched together into one'. " "Also dictated by your insurance coverage that doesn't want to cover anything that costs money." "The nursing shortage in the ER is real. The other night in my large ER, the most senior nurse we had was two years into his nursing career." "Unless you are in a union shop with mandated staffing ratios, your hospital is not staffing enough nurses and aides to take care of you safely and comfortably. To save money." "Each specialty in the hospital is funded differently according to the money they bring in. Because of this, the emergency room is constantly losing money — hence, budget cuts, hence, unsafe staffing and care." "I just want to be a nurse: with equipment that works, supplies available (instead of tying the IV bag onto the broken bed pile with a tourniquet), and a nurse-to-patient ratio that I can not only have the time to give my patients outstanding care, but also be able to have the time to grab them a blanket or a sandwich. But I can't when one room is hemorrhaging from a complicated miscarriage, I'm adjusting someone's IV meds every 10 minutes so their heart rate doesn't jump into the 200s again, I'm doing every 15 neuro checks on a stroke patient — oh, but the 25 year old who's belly pain that turns out to be constipation and was told by the doctor that they are being discharged is furious because it's taking too long to get their discharge paperwork because 'they haven't eaten in, like, forever.'" "Liability and profitability are the main drivers shaping your health plan, not medical research and expertise. The insurance industry is ultimately the decision maker in healthcare for the general public, and they don’t care whether it benefits you." "There have been multiple studies that show higher patient satisfaction is tied to higher mortality." "These same doctors a lot of times are a NIGHTMARE in the OR. Mean as hell to staff, yelling, cussing. But sure, your prayer with the patient in preop means you are 'one of the good ones.'" "Being compassionate for patients doesn't equal clinical outcomes. The 'most caring' physicians can often be very poor performers clinically, whereas some of the 'greedy' physicians I would vastly prefer to take care of me, knowing their outcomes." "I think people tend to forget that healthcare practitioners are still people and not all people are top of their class or great at their jobs. I still trust all of you more than I'd trust anyone else to administer medical attention, but it's also really important to get second opinions just in case."
Comments
You must be logged in to comment.